A woman in her 50s, who developed a vesicovaginal fistula after undergoing surgery for uterine fibroids, had previously undergone a repair procedure but experienced recurrence and urinary incontinence.
Today, we performed a laparoscopic repair procedure.
This was her third surgery, and since omentum had been used in the previous repair, adhesion dissection was a critical aspect of the procedure.
The sigmoid colon, omentum, and ileum were adhered to the pelvic floor, with the adhesion of the sigmoid colon being particularly challenging and requiring careful attention.
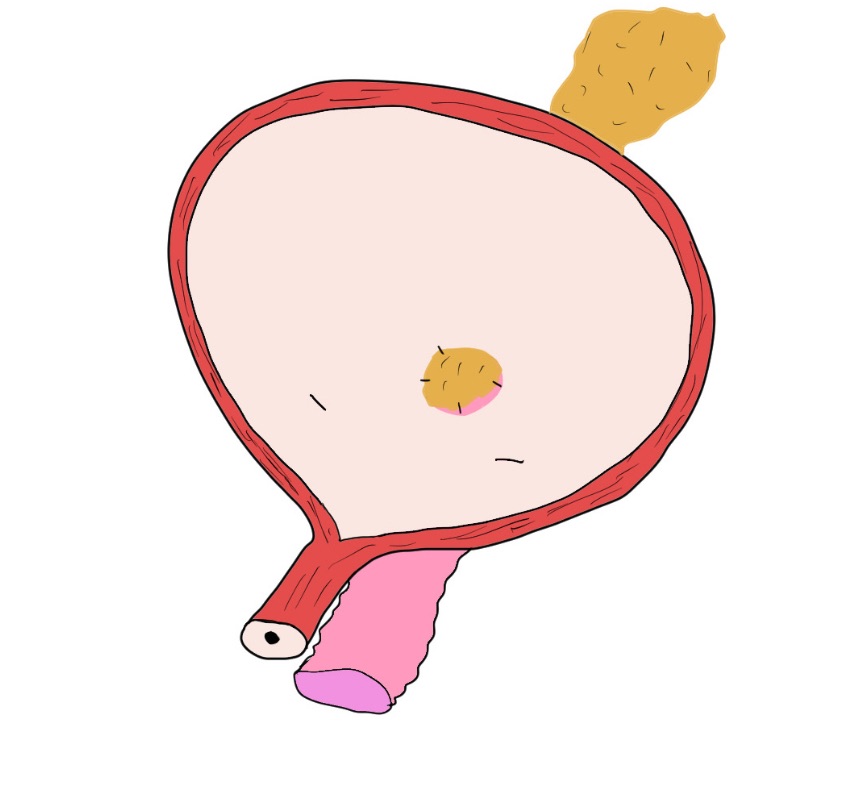
We confirmed the position of a catheter that had been pre-inserted from the vagina to the bladder. The unhealthy tissue around the fistula was excised, and the bladder was sutured in two layers—mucosa and muscle layer—while the vaginal wall was closed in a single layer. Additionally, adipose tissue from the lateral side of the bladder was placed between the bladder and the vaginal wall. This adipose tissue, with its excellent blood supply, is highly beneficial for tissue healing and also helps absorb exudates.
I wrote this with the hope that urologists might find it useful in understanding how to approach such repairs.
I understand that some doctors may hesitate to proceed with follow-up or treatment, or may find it daunting to seek consultation. However, I would like to encourage my colleagues in urology and gynecology to feel free to reach out for advice or support.
We also offer short-term hospital stays, such as a 3-night, 4-day program, for this procedure.
#Kameda medical center
