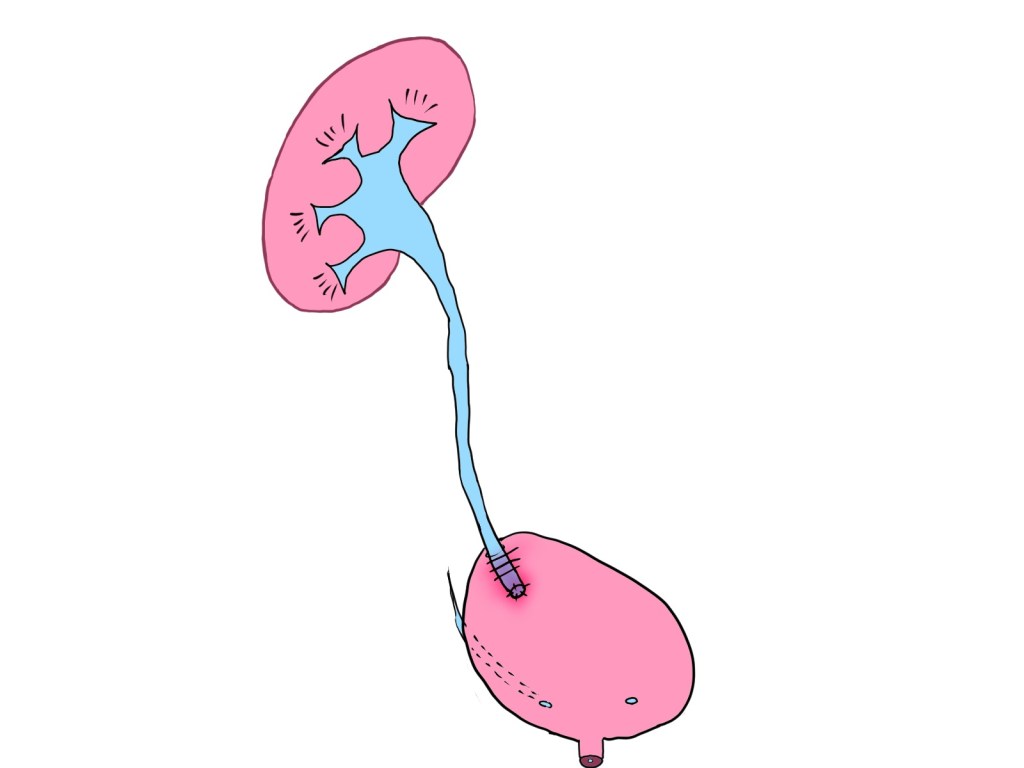
Today, I performed surgery at Kameda Medical Center for a woman in her 30s who developed a ureterovaginal fistula following a laparoscopic hysterectomy.
We opted for a laparoscopic ureteral reimplantation, utilizing the psoas hitch technique and constructing a submucosal tunnel to prevent vesicoureteral reflux.
Background: Ureteral Injury and Its Mechanism
The site of ureteral injury was at the crossing with the cardinal ligament, where the tissue showed circumferential degeneration and severe adhesion to surrounding structures.
Given the appearance, it was most likely caused by thermal injury from a sealing device used during the initial procedure.
While medical devices have advanced tremendously, inappropriate use can lead to serious complications like this one.
Surgical Considerations and Techniques
Key intraoperative strategies included:
• Meticulous dissection to separate adhesions from adjacent organs
• Selection of ureteral segment with good blood flow and adequate length
• Creation of a submucosal tunnel of appropriate length and angle to prevent reflux
• Tension-free anastomosis with precise suturing to avoid leakage
A Learning Experience for All
This was a joint procedure with a young trainee surgeon.
The operation was filled with excellent questions:
“Where exactly do we fix the ureter in a psoas hitch?”
“How long should the submucosal tunnel be?”
Answering these real-time inquiries added a valuable educational element and highlighted the trainee’s growth.
No Matter How Technology Evolves, Basics Remain Essential
With the rise of laparoscopic and robot-assisted surgeries, it’s easy to rely on machines.
But this case reminded us that “seeing, feeling, and judging with our own eyes and hands” remains the foundation of safe and effective surgery.
Every case like this reinforces one truth:
Technology doesn’t replace technique — it amplifies it when used wisely.
